Moving towards
3D Bioprinted Cardiovascular Tissue
By Dr Ivan De Backer,
Technology Analyst, IDTechEx
Alenka joined Johnson & Johnson more than 20 years ago and has held several roles of increasing local and regional responsibility across Johnson & Johnson sectors.
In her current role, Alenka leads Biosense Webster, Cerenovus and Mentor companies which develop innovative technologies in the field of cardiac arrhythmias treatment, ischemic and hemorrhagic stroke treatment and breast surgery.
Alenka holds an Economics degree from the University of Ljubljana and obtained her MBA from Hofstra University in New York. She resides in Slovenia with her family.
Alenka Brzulja
Vice President of Cardiovascular & Specialty Solutions EMEA, Johnson & Johnson Medical Devices Companies.
- Iaizzo PA (2015). Handbook of Cardiac Anatomy, Physiology and Devices. Springer Science and Business Media, LLC: Switzerland.
- Odutayo A et al. (2016) Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and meta-analysis. BMJ 354:i448
- Aliot E, et al. (2010) An international survey of physician and patient understanding, perception, and attitudes to atrial fibrillation and its contribution to cardiovascular disease morbidity and mortality. Europace 12 (5): 626-63
- Zoni-Berisso M, Lercari F, Carazza T, Domenicucci S (2014) Epidemiology of atrial fibrillation: European perspective. Clin Epidemiol 6 213-220.
- Ball J, Carrington MJ, McMurray JJ, Stewart S. Atrial fibrillation: profile and burden of an evolving epidemic in the 21st century. Int J Cardiol 2013;167(5):1807–24.
- Abed, H. S. and Wittert, G. A. (2013), Obesity and atrial fibrillation. Obes Rev, 14: 929–938.
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D et al. (2016) 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 37 (38): 2893-2962.
- Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y et al. (2009) Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm Electrophysiol 2 (4): 349-361
- Pillarisetti J, Lakkireddy D. Atrial fibrillation in Europe: state of the state in disease management! Bloch Heart Rhythm Center, Division of Cardiovascular Diseases, Cardiovascular Research Institute, University of Kansas Hospital & Medical Center, Kansas City, KS. European Heart Journal (2014) 35, 3326–3327
- Kuck KH, Lebedev, D., Mikaylov, E., Romanov, A., Geller, L., Kalejs, O., Neumann, T., Davtyan, K., On, Y.K., Popov, S., Ouyang, F. (2019) Catheter ablation delays progression of atrial fibrillation from paroxysmal to persistent atrial fibrillation. ESC Late-breaking Science 2019. Paris, France. August 31, 2019.
- Hussein A, Das M, Chaturvedi V, Asfour IK, Daryanani N et al. (2017) Prospective use of Ablation Index targets improves clinical outcomes following ablation for atrial fibrillation. J Cardiovasc Electrophysiol 28 (9): 1037-1047.
- Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD et al. (2019) Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA
- Mark DB, Anstrom KJ, Sheng S, Piccini JP, Baloch KN et al. (2019) Effect of Catheter Ablation vs Medical Therapy on Quality of Life Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA
- Jais P, Cauchemez B, Macle L, Daoud E, Khairy P et al. (2008) Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation 118 (24): 2498-2505
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB et al. (2017) 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 14 (10): e275-e444.
References


Dr. Ivan De Backer is a Technology Analyst at IDTechEx. His main activities include conducting target assessments, market forecasts and key player analysis for the delivery of research reports and consulting projects. Ivan works in the field of Life Sciences and is interested in emerging and innovative technologies from all areas of the medical industry. He obtained his PhD in Clinical Medicine from Imperial College London and holds a BSc in Pharmacology from the University of Bath, UK. Ivan has a background in medical research, having previously worked as a laboratory scientist within the pharmaceutical industry in the fields of neurodegenerative diseases, schizophrenia and metabolic disorders.
Cardiovascular disease (CVD) is the leading cause of death worldwide, with over 17 million per year according to the World Health Organisation. Many forms of CVD are chronic in nature, meaning that they worsen over time. Thus, once the disease has been diagnosed it is important to initiate treatment as soon as possible in order to provide positive patient outcomes.
The ideal treatment for some forms of severe CVD, such as chronic heart failure or extensive myocardial injury, is cardiac transplantation. Due to shortages in available donor tissue, this cannot be given to all patients. The average waiting time for a suitable donor is six to twelve months in the USA and around one in six people die before they can receive a transplant. There is a clear need for a more abundant supply of hearts suitable for transplantation.
Until significant progress has been made to boost this supply, cardiologists need to rely on the technology at their disposal. A common strategy to address heart failure is to use a cardiac pump such as a left ventricular assist device (LVAD). Mechanised hearts have also been explored as a treatment option for chronic heart failure when transplant donors are not available.
Current treatment options are useful to a certain extent, but personalised solutions are required to improve patient outcomes and quality of life. This need is driving the development of cardiovascular 3D bioprinting technologies, which make use of 3D printing-like techniques to combine cells and biomaterials to fabricate biomimetic structures that replicate natural tissue physiology and function.
Developing a dynamic cardiac tissue capable of mimicking the mechanical and electroconductive properties of native myocardium is proving difficult to researchers. Many challenges stand in their way including, among others, re-creating tissue matrix and providing an adequate oxygen supply to each cell.
The success of 3D bioprinting depends on researchers’ ability to vascularise the tissue. For this reason, a lot of focus has recently been placed on the generation of blood vessels. Several promising studies have already been conducted. For instance, researchers at University of California San Diego 3D printed a functional blood vessel network which, once implanted in mice, merged with the animal’s blood vessels and was capable of transporting blood. Similar achievements have been reported by Sichuan Revotek, Rice University and the University of Pennsylvania in the last few years.
An important innovation as we move towards 3D bioprinting cardiac tissue is the development of cell sheets. Terumo, a Japanese conglomerate, has commercialised the Heart Sheet for treatment of heart failure in Japan. To develop Heart Sheet, muscle tissue is harvested from the patient’s leg and cultured in vitro. Terumo has developed a tissue culture plate that allows cells to float off the surface in an intact sheet when the temperature is lowered, thus preserving the extracellular matrix that is lost when cells are removed by other methods.
Cardiac tissue engineering techniques such as this one can be used to create functional constructs capable of re-establishing the structure and function of damaged myocardium following myocardial infarction. The engineered cardiac tissue, which often comes in the form of a “patch”, is implanted directly onto scar tissue. The intention is to compensate for the heart’s reduced function by strengthening its structure and boosting its ability to pump blood. This way, researchers hope to reduce the need for transplants, improve recovery and prevent subsequent events.
Researchers across the world are developing “cardiac patches”. In June 2019, Imperial College London announced the creation of thumb-size patches of heart tissue that start to beat spontaneously after three days and start to mimic mature heart tissue within one month. These patches successfully led to improvements in heart function following a heart attack after only four weeks. Importantly, blood vessels appeared to have formed within the patch after that time. Clinical trials are expected to be held in 2020 or 2021.
Once implanted, cardiac patches could do more than just promote cardiac tissue regeneration. For instance, a bionic patch could deliver electrical shocks and act as a pacemaker. Scientists at the University of Tel Aviv also investigated integrating electronic sensors into the patch to enable remote monitoring of cardiac activity.
Although researchers have not yet been able to create a fully functioning artificial heart, an important leap was made in 2019. Researchers from Tel Aviv University unveiled the first 3D bioprinted heart with human tissue including chambers, ventricles and blood vessels. To accomplish this, a biopsy of fatty tissue from patients was taken to produce the cells required. Patient-specific cardiac patches were produced first, after which the entire heart was made. Although the heart is capable of contracting, it remains a long way off from being ready for clinical trials as it cannot yet pump blood and is the size of a cherry.
3D bioprinting has the potential to provide a heart or blood vessels to patients in need of transplants. The tissue would be made from their own cells, thereby considerably reducing the risk of rejection. Despite promising recent innovations, 3D bioprinting technology remains in its early days and is unlikely to become a viable therapeutic option in the near future due to the numerous roadblocks (both technical and regulatory) that it currently faces. This will change once the technology evolves and full-sized hearts and vessels can be constructed efficiently and at scale.
To find out more about technologies for 3D bioprinting cardiovascular tissue, or on the topic of cardiovascular disease management as a whole, please refer to IDTechEx’s report: “Cardiovascular Disease 2020-2030” available on the IDTechEx website at www.IDTechEx.com/CVD

Moving towards 3D bioprinting cardiovascular tissue
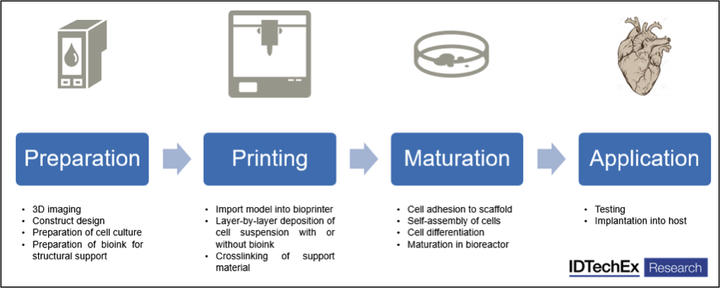
The process of 3D bioprinting





