

3-Dimensional Echocardiography in Transcatheter Tricuspid Valve Interventions
Dr. Stamatios Lerakis joined the Zena and Michael A. Wiener Cardiovascular Institute as full-time faculty on September 1st 2018, in the role of Professor of Medicine and Director of Noninvasive Cardiology for Mount Sinai Heart and the Director of Imaging for Structural and Valve Interventions for the Mount Sinai Health System. He is a recognized multimodality cardiac imager and an international expert in imaging for Structural and Valve Interventions. Dr. Lerakis, in collaboration with the NIH, has guided the first in humans Transcatheter Mitral Valve Replacement After Transcatheter Electrosurgical Laceration of Alfieri STItCh (ELASTIC), the first in humans Intentional Percutaneous Laceration of the Anterior Mitral Leaflet to Prevent Outflow Obstruction During Transcatheter Mitral Valve Replacement (LAMPOON) and the first in humans single and double Bioprosthetic Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction (BASILICA) during TAVR. He received his M.D. degree from the Medical School of Athens (Greece). He continued on doing clinical research in Nuclear Cardiology at Mount Sinai Hospital. Subsequently, he did his Internal Medicine training in the Presbyterian Medical Center of Philadelphia and then completed a year of Fellowship in Critical Care in Brown University. He went on to complete his Cardiology Fellowship at the University of Texas Medical Branch in Galveston, Texas and then did one year of Echocardiography Fellowship at Emory University. After his Echocardiography Fellowship, he stayed on as Faculty in the Division of Cardiology at Emory University where he was Professor of Medicine, Radiology and Imaging Sciences, Director of Imaging for the Structural and Valve interventions in Emory Healthcare, the Medical Director for Nuclear Cardiology and Cardiac MRI at Emory University Hospital and Emory Clinic, as well as the Fellowship Program Director for the Advanced Cardiovascular Imaging Fellowship (CMR and CCT) and he initiated and established the Fellowship for Imaging for Structural and Valve Interventions.
Stamatios Lerakis, MD
Director of Imaging for Structural and Valve Interventions for the Mount Sinai Health System
Stamatios Lerakis,
MD, PhD
Director of Imaging for Structural and Valve Interventions for the Mount Sinai Health System
Structural Imaging Fellow, Division of Cardiology, Icahn School of Medicine at Mount Sinai
MD FACC
Richard Ro,
Dr. Richard Ro received his M.D degree at Stony Brook School of Medicine in conjunction with the Sophie Davis School of Biomedical Education at the City College of New York. He completed his Internal Medicine training at Rutgers-Robert Wood Johnson University Hospital in New Brunswick, New Jersey and subsequently did an Echocardiography/Nuclear Cardiology fellowship at Mount Sinai St. Luke’s-Mount Sinai West Hospitals in New York. He remained there for his general cardiology fellowship, and after its completion, pursued a fellowship in Structural Imaging at Mount Sinai Hospital, where he currently is the inaugural fellow under the guidance of Dr. Lerakis.
Richard Ro, MD FACC
Structural Imaging Fellow, Division of Cardiology, Icahn School of Medicine at Mount Sinai
The tricuspid valve has an intricate configuration with its function dependent on the synchronized coordination of its various component.1 The occurrence of significant tricuspid regurgitation (TR) because of the dysfunction of the valve apparatus or its surrounding structures is linked with dismal clinical outcomes.2,3 The rapid emergence of transcatheter procedures, which are currently being actively investigated, can offer a non-surgical treatment pathway in the management of severe tricuspid regurgitation.4 Three-dimensional (3D) echocardiography plays an important role in the initial diagnosis and eventual interventional procedural guidance for these patients.
In the transthoracic exam, 3D images may be beneficial and informative given the anterior location of the right–sided cardiac structures in the chest, allowing for simultaneous visualization and identification of all three tricuspid leaflets and etiology of regurgitation. The commissure between the anterior and septal leaflets is generally close in proximity to the non-coronary cusp of aortic valve, and the coronary sinus is near the commissure between the septal and posterior leaflet. These landmarks, in addition to the interventricular septum and aortic valve, can aid in identifying each individual leaflet. Transesophageal echocardiography is then performed in these patients. 3D imaging in the midesophageal and transgastric views while focusing on the tricuspid valve should be attempted if the two-dimensional images are of sufficient quality. In our experience, the bicaval view in full volume mode is particularly useful to view the tricuspid valve en-face in relation to the interatrial septum and aortic valve, which aids in the identification of the leaflets. Color Doppler should be applied to all 3D images to identify the origin and directionality of the regurgitant jet. (Figure 1)
During transcatheter intervention of the tricuspid valve, transesophageal echocardiography is primarily used, although intracardiac echocardiography can be used in more difficult cases. A combination of 2D and 3D imaging is used for clip steering and navigation, appropriate clip positioning between the two targeted tricuspid leaflets, confirmation of adequate leaflet grasping, and subsequent reduction of tricuspid regurgitation.
Several transcatheter devices are currently undergoing investigation for severe TR in a number of clinical trials.4,5 A set of standardized and reproducible multimodality imaging algorithms, consisting of computed tomography, echocardiography with transthoracic (TTE) and transesophageal (TEE) approaches, that can be used to image the anatomical and functional nature of the tricuspid valve, as well for intra-procedural device navigation, will ultimately be necessary as transcatheter treatment of TR continues to expand.6
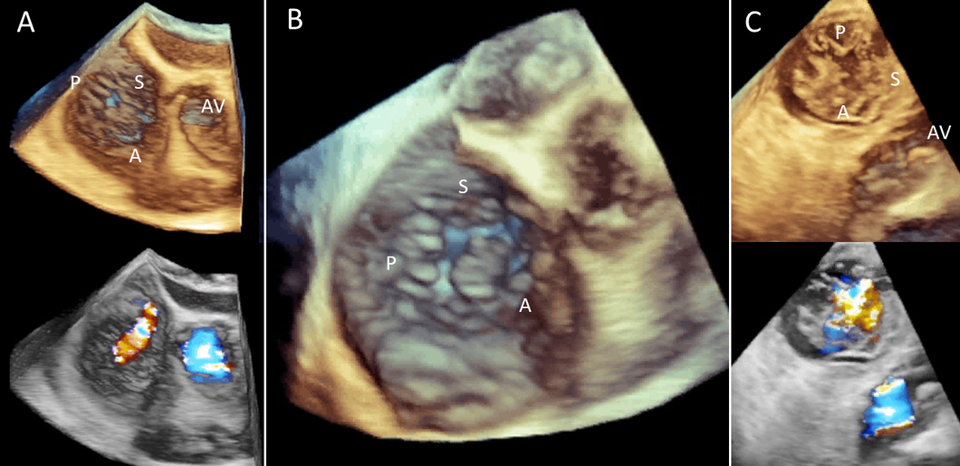
Figure 1:
A. Transesophageal echocardiography with full volume imaging from the midesophageal bicaval view with corresponding color Doppler below. The anterior (A), posterior (P), and septal (S) leaflets are shown, as well as the aortic valve (AV).
B. This 3D TEE view at the same echocardiographic window is once again noted with leaflet identification using surrounding anatomical landmarks.
C. In a 3D image from the transgastric view on TEE, the three leaflets can again be clearly identified including the aortic valve (AV). Corresponding color Doppler below shows the tricuspid regurgitant jet (orange), as well as aortic outflow jet (blue).
References
- Huttin O, Voilliot D, Mandry D, Venner C, Juilliere Y, Selton-Suty C. All you need to know about the tricuspid valve: Tricuspid valve imaging and tricuspid regurgitation analysis. Arch Cardiovasc Dis. 2016;109:67-80.
- Dahou A, Levin D, Reisman M, Hahn RT. Anatomy and Physiology of the Tricuspid Valve. JACC Cardiovascular Imaging. 2019;12:458-68.
- Zack CJ, Fender EA, Chandrashekar P, Reddy YNV, Bennett CE, Stulak JM, Miller VM, Nishimura RA. National Trends and Outcomes in Isolated Tricuspid Valve Surgery. J Am Coll Cardiol. 2017;70:2953-60.
- Hahn RT, Nabauer M, Zuber M, Nazif TM, Hausleiter J, Taramasso M, Pozzoli A, George I, Kodali S, Bapat V, Maisano F. Intraprocedural Imaging of Transcatheter Tricuspid Valve Interventions. JACC Cardiovasc Imaging. 2019;12:532-53.
- Hahn RT. State-of-the-Art Review of Echocardiographic Imaging in the Evaluation and Treatment of Functional Tricuspid Regurgitation. Circ Cardiovasc Imaging. 2016;9:1-14.
- Ro R, Tang GHL, Seetharam K, Khera S, Sharma SK, Kini AS, Lerakis S. Echocardiographic Imaging for Transcatheter Tricuspid Edge-to-Edge Repair. J Am Heart Assoc. 2020 Mar 3;9(5):e015682. doi: 10.1161/JAHA.119.015682. Epub 2020 Feb 24.
References


