Catheter Precision
Planning Ventricular Ablation with Confidence
By Stephanie Kreml
Catheter Precision’s VIVO mapping system identifies the origin of ventricular arrhythmias noninvasively with no special equipment so EP's can confidently plan their ablation procedures.



A Shift from Robotics
Ventricular ablation procedures are long and complex. Localizing the area(s) to ablate throught catheter based cardiac consumes most of the time it takes to do the procedure. And even then, outcomes may be poor, particularly in patients with structural heart disease.
With Catheter Precision’s VIVOTM (View into Ventricular Onset) mapping system, cardiac electrophysiologyst (EPs) have the information they need to improve the planning of their ventricular ablation procedures, saving hours of time and potentially improving patient outcomes.
Although VIVO is pushing the envelope of cardiac imaging, Catheter Precision’s roots are in robotics. “The company was originally called Catheter Robotics and initially developed the Amigo®Remote Catheter System, a robotic device for placement of catheters for EP procedures,” says CEO Steve Adler. “VIVO is our second product and expanded our product offerings into mapping.”
And with VIVO, the company is now focusing on ventricular arrhythmias, helping electrophysiologists improve their efficiency during the ablation procedure.
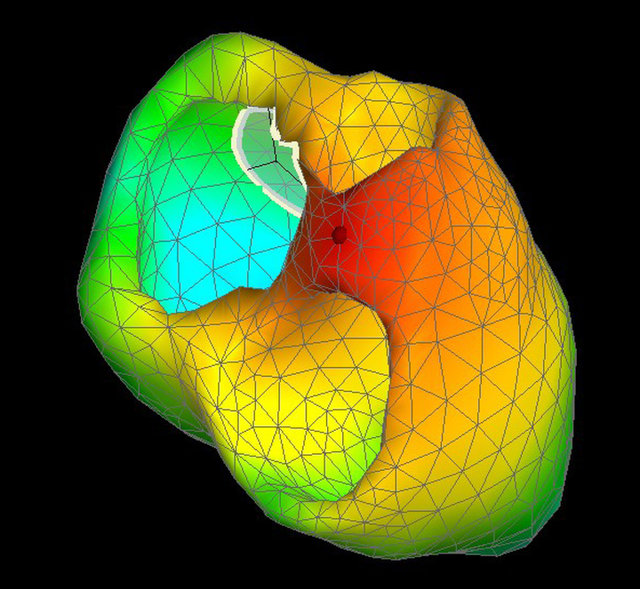
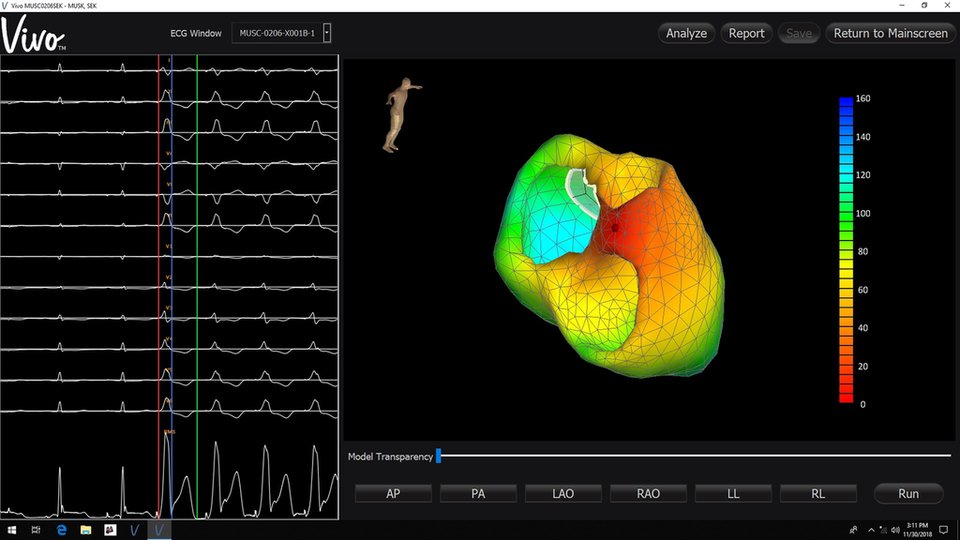
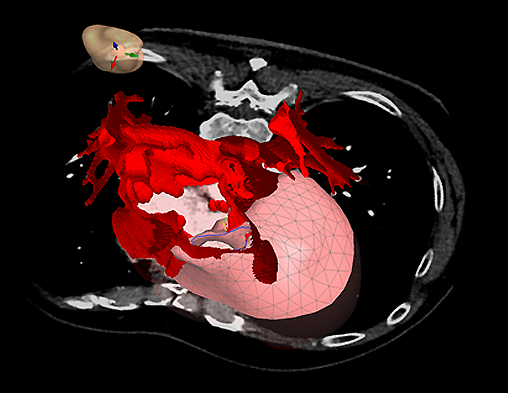
“The VIVO system is a noninvasive pre-procedure planning tool that provides a 3D mapping of the heart to aid in the identification of the general location of the origin of cardiac arrhythmias,” Adler explains. “VIVO requires acquisition of MRI or CT images and standard ECG recordings and lead placement.” To more precisely locate the ECG leads along with a set of Position Patches on the patient’s torso, the system also uses images from an off-the-shelf 3D camera.
“Electrocardiographic potentials are measured from the torso using standard 12 lead electrocardiograph (ECG) leads placed on the surface of the body,” Adler says. “A DICOM image (CT or MR scan) of the thorax and heart is acquired and then segmented to provide a detailed, three-dimensional anatomy of the endocardial and epicardial surface of the heart.” After the cardiology team captures all these data, they are uploaded into Catheter Precision’s platform. The system merges the 3D chest images with the DICOM CT or MR data to “determine the spatial relationship between the electrodes and the heart.”
The system then uses mathematical models to deduce the origin of the arrhythmia. Adler describes the process, “From these data, the system uses a mathematical algorithm to use the geometrical information to transform the measured body surface potentials into myocardial potentials via a unique solution to the cardiac inverse problem.” These are tried and true methods that do not rely on the new wave of artificial intelligence. He points out, “At this time, VIVO’s algorithms are based on proven electrophysiology methods and calculations, such as the inverse solution, and do not incorporate AI into the technology. However, research is being conducted into using AI solutions to improve performance"
Simplifying the Complex
The concept of using external electrodes to determine the origin of ventricular arrhythmias is not completely new. But VIVO’s closest competitor, CardioInsight by Medtronic, requires special equipment to capture hundreds of signals to perform its calculations. “VIVO’s advantage is lower cost and simplicity with using a standard 12-lead ECG versus a 250+ electrode body surface potential map,” Adler says.
And he doesn’t believe VIVO will displace intra-procedural catheter mapping for now. “VIVO simplifies and shortens procedure time, but still requires confirmatory mapping using a mapping computer,” Adler states. “In fact, VIVO’s output can be superimposed on their machines to improve guidance during the procedure.”
This approach can improve and electrophysiologist’s confidence during ablation. “The accuracy of the VIVO system has been shown to be 100% accurate (95% CI: 93.6%, 100%) in a prospective multi-center clinical trial,” Adler affirms. These studies showed the system could identify PVC or VT foci in the right, left, or septal regions of the heart.
Improving Efficiency
Now that VIVO received FDA clearance last summer, Adler believes the system is set to improve ventricular ablation procedures by making them faster, less complex, more effective, and less expensive.
Since EP's spend most of the procedure time mapping the heart to identify the origin of the arrhythmic signals, this can be greatly reduced. “By having pre-procedure VIVO localization information followed by confirmatory mapping, procedure time should be reduced by up to 75%,” Adler says.
The additional pre-procedure information VIVO provides electrophysiologist helps them improve their planning. Adler explains, “For example, if VIVO localized to the right side of the heart, then the staff can plan for a shorter procedure without the complexities involving the left side of the heart.”
Using VIVO may decrease procedure failure rates, even though it is not altering the delivery of energy during ablation. “Better and more accurate identification of the arrhythmic origin as well as better procedure planning may lead to improved outcomes,” says Adler.
And finally, using VIVO may decrease the cost of the procedure. “[P]re-procedure planning would allow a shorter procedure, the potential to know exactly what intracardiac devices are needed (i.e. only opening one catheter) and the ability to perform more cases in the same amount of time,” Adler concludes.
Catheter Precision continues work to expand indications for VIVO. One area where VIVO may be used is to guide physician lead placement for bi-ventricular and HIS-Bundle pacing. “Bi-ventricular pacing or cardiac resynchronization therapy has an approximate 35% failure rate that I believe can be improved with better tools, such as VIVO,” Adler says.
And VIVO may circle back to improve the performance of Catheter Precision’s original robotic system. “Eventually, I believe that VIVO can become the guidance system for an Amigo-like robot which can deliver catheters to various locations in the heart on demand.”
By having pre-procedure VIVO localization information followed by confirmatory mapping, procedure time should be reduced by up to 75%.
Guiding the Future


Pre-procedure planning would allow a shorter procedure, the potential to know exactly what intracardiac devices are needed and the ability to perform more cases in the same amount of time.
Steve Adler, CEO, Catheter Precision